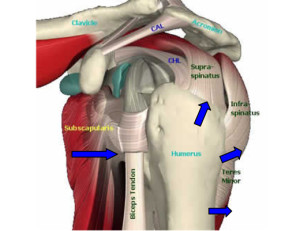
 The shoulder is made up of three bones: the upper arm bone (humerus), the shoulder blade (scapula), and the collarbone (clavicle). The shoulder is a ball-and-socket joint: The ball, or head, of the upper arm bone fits into a shallow socket in the shoulder blade. The arm is kept in the shoulder socket by the rotator cuff. The rotator cuff is a network of four muscles that come together as tendons to form a covering around the head of the humerus. The rotator cuff attaches the humerus to the shoulder blade and helps to lift and rotate the arm.
The shoulder is made up of three bones: the upper arm bone (humerus), the shoulder blade (scapula), and the collarbone (clavicle). The shoulder is a ball-and-socket joint: The ball, or head, of the upper arm bone fits into a shallow socket in the shoulder blade. The arm is kept in the shoulder socket by the rotator cuff. The rotator cuff is a network of four muscles that come together as tendons to form a covering around the head of the humerus. The rotator cuff attaches the humerus to the shoulder blade and helps to lift and rotate the arm.
There is a lubricating sac called a bursa between the rotator cuff and the bone on top of the shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when the move your arm. When the rotator cuff tendons are injured or damaged, this bursa can also become inflamed and painful.
When one or more of the rotator cuff tendons is torn, the tendon no longer fully attaches to the head of the humerus. Most tears occur in the supraspinatus muscle and tendon, but other parts of the rotator cuff may also be involved. In many cases, torn tendons begin by fraying. As the damage progresses, the tendon can completely tear, sometimes with lifting a heavy object. The fraying is caused by too much tension or an imbalance in the muscles which needs to be corrected.
Causes of a rotator cuff injury may include falling, lifting and repetitive arm activities — especially those done overhead, such as throwing a baseball or placing items on overhead shelves. Repetitive use and/or improper body mechanics can also lead to injury. As we age and become less active we tend to lose strength and tendons begin to breakdown. Rotator Cuff Injuires are most common in people over 40 years old. There is a very good chance that a rotator cuff injury provided it is not severely torn, can heal with self-care measures or exercise therapy
Rotator cuff injury signs and symptoms may include:
Pain and tenderness in the shoulder, especially when reaching overhead, reaching behind the back, lifting, pulling or sleeping on the affected side
Shoulder weakness
Loss of shoulder range of motion
Inclination to keep the shoulder inactive
The most common symptom is pain. It may occur when reaching up to comb hair, bending the arm back to put on a jacket or carry something heavy. Lying on the affected shoulder also can be painful. If a severe injury, such as a large tear, has occurred there can be continuous pain and muscle weakness.
So our primary goal is to release scar tissue that has formed following injury, restore ranges of motion and regain stability. Torn muscles, most commonly the supraspinatus (on the top of the shoulder blade), create general instability in the shoulder joint. Once range of motion has been restored, strength will be required to fully resolve the injury and prevent the problem from becoming chronic (i.e. frozen shoulder).
The manner in which the treatment is tailored depends on which muscle is torn. Make sure to determine the exact injury and tailor the treatment accordingly. If your client is very apprehensive about stretching the shoulder, begin with strength training (i.e, manual resistance and ROM movements) to establish confidence and stability. Once initial gains in stability have been attained you will have greater success doing the stretching protocols. This is especially true for dislocations.
Make sure to pay attention to the client’s reactions both emotional and physical. Work with the client and address their issues as you go.
So how would I work with A Rotator Cuff Injury:
I would use the following Stretching protocol
Shoulder Horizontal Abduction
Shoulder Extension
Shoulder Internal Rotation
Shoulder External Rotation
Shoulder Horizontal Adduction
Shoulder Abduction
Posterior Hand Clasp
I would then proceed to opening up the cervical area with another series of stretches. Once I have the client out of pain and confident that they can in fact use their shoulder I would introduce strengthening exercises. Starting with a light manual resistance and gradually moving up to weights. I am also massaging (in between stretches – gives the client a break and brings their awareness to the changes in the soft tissue) and treating trigger points as they arise. Finally I would review the client’s body mechanics and try to correct improper use that is contributing to the problem. The client would be given a protocol do follow at home with daily shoulder stretches and a shoulder-strengthening to help prevent a recurrence. Especially important is a program of strength exercise to promote balanced strength about the shoulder.
So now you know my approach I would love to hear yours! Please share how you view and treat the Rotator Cuff.